NEWS FROM KAROLINSKA INSTITUTE
It is possible to leave most lymph nodes in the armpit – even if one or two of them contain metastases larger than two millimeters. This is shown by a study involving women from five countries, led by Karolinska Institutet and published in the prestigious journal New England Journal of Medicine. The study opens the way for more gentle surgery for breast cancer patients.
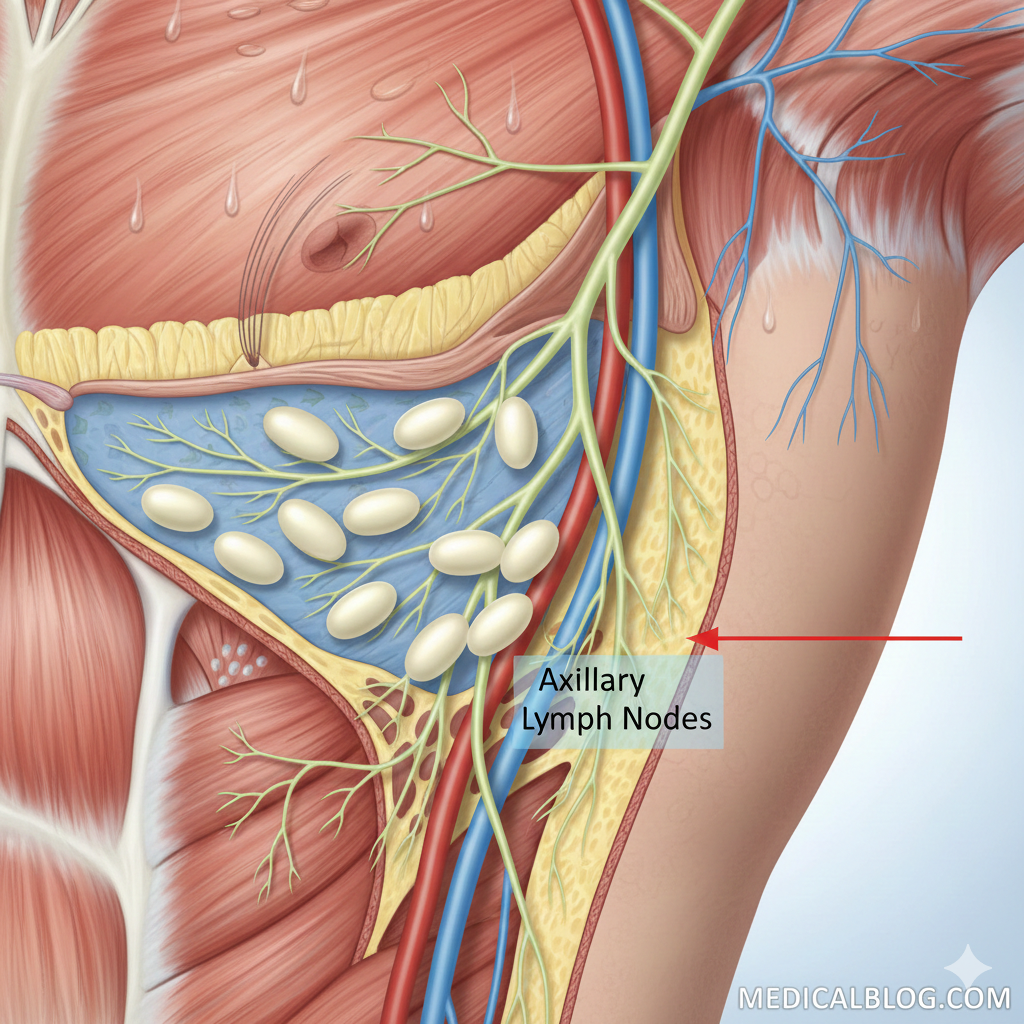
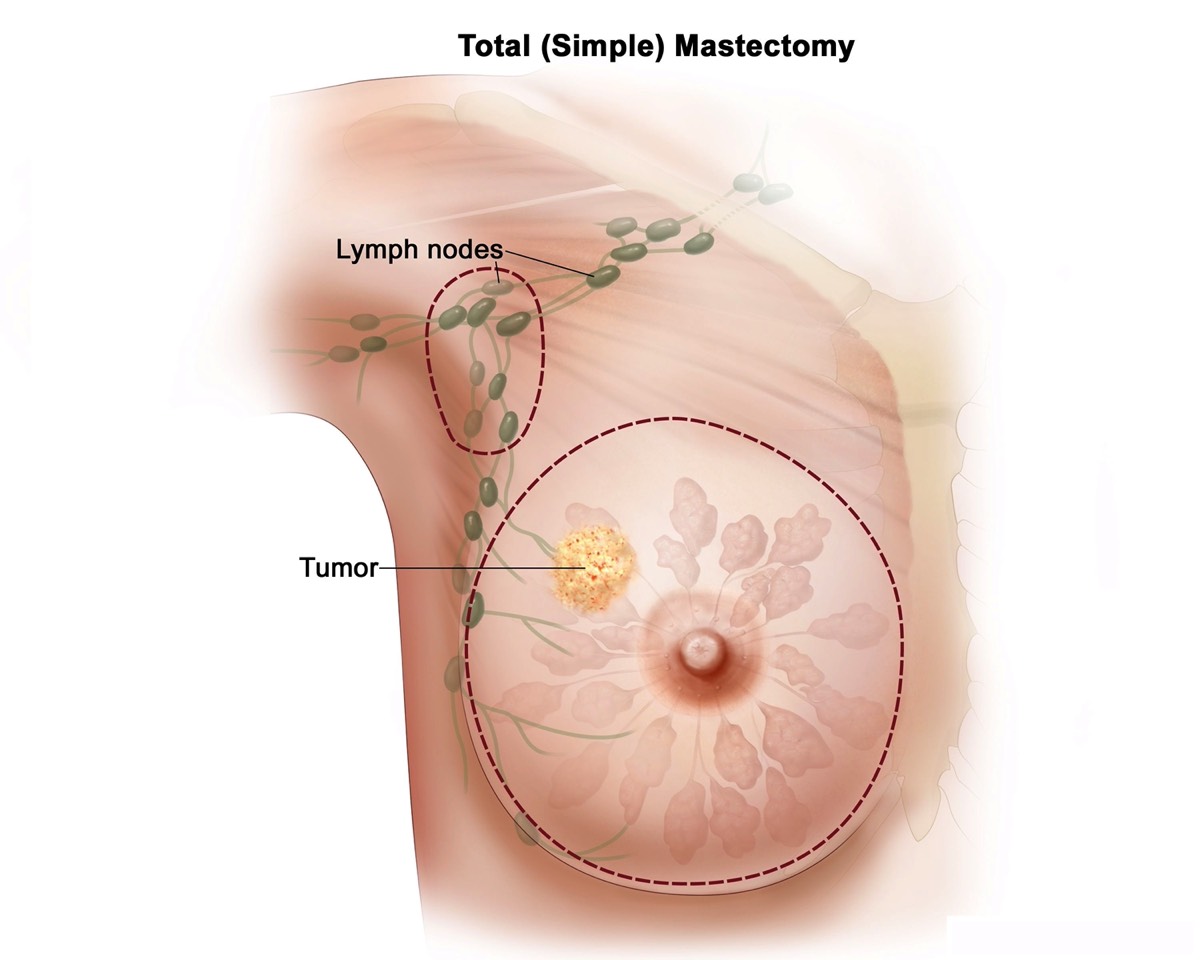
Breast cancer can spread to the lymph nodes in the armpit. However, tumors in only the breast and armpit lymph nodes are considered local disease, where the goal is for the patient to be cured.

A difficult question for breast cancer surgeons is what should be done when patients have metastases in the armpit, which are only discovered during examination of tissue removed during surgery.
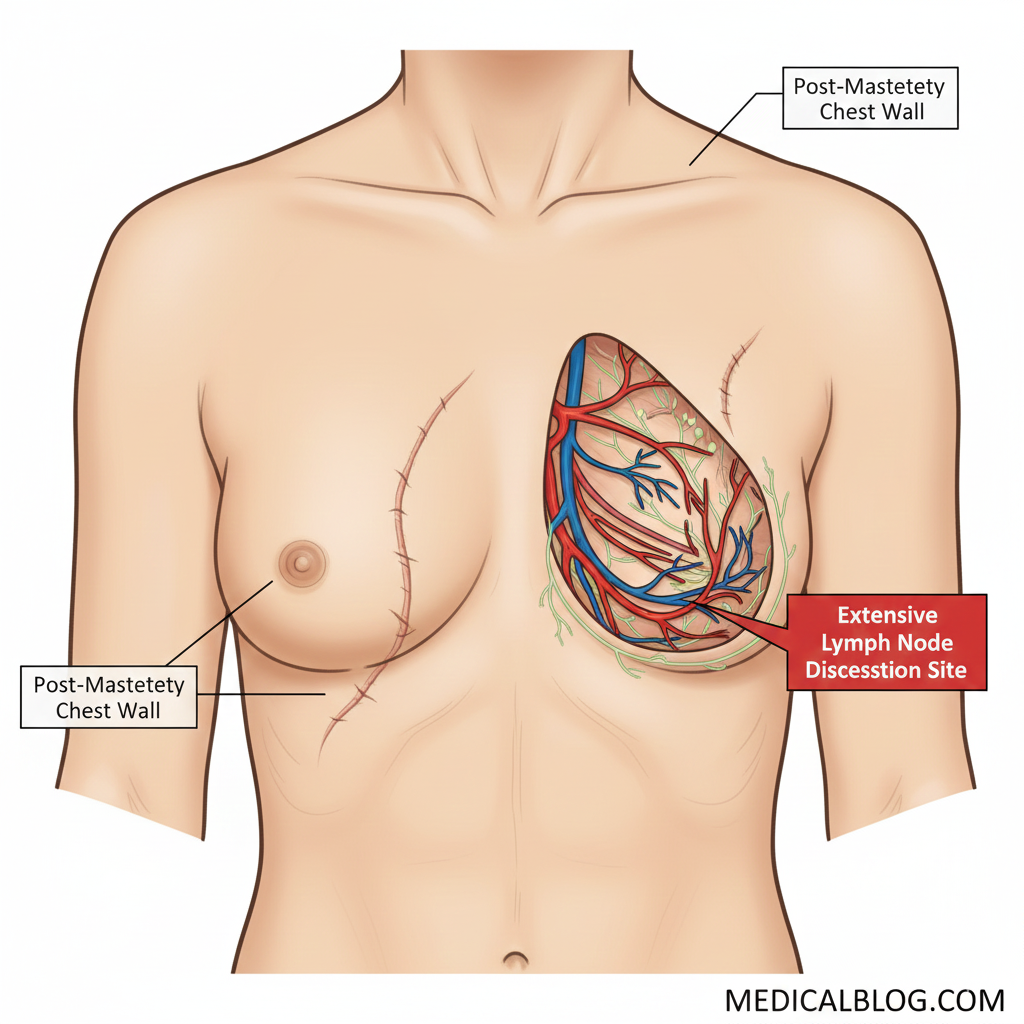
Having an axillary dissection (removing many lymph nodes in the armpit) increases the risk of lymphedema in the arm. This occurs when lymph fluid cannot flow as freely as before. This can cause swelling in the arm, pain, and affect mobility.
When it is known even before breast cancer surgery that there are metastases in the armpit, various treatment options fall into place. These patients are not included in this study.
However, when no spread is known, the surgeon usually removes the so-called sentinel glands (the gland or glands that are first reached by lymphatic fluid from the breast).
Safely leaving lymph nodes.
If they contain single tumor cells or metastases measuring no more than 2 millimeters, the rest of the lymph nodes in the armpit are left intact.
Previous studies have shown that this is safe for the patient.
Now, extensive research led by Karolinska Institutet has clarified the situation even for larger metastases.
The study includes nearly 2,800 patients from five different countries.
All had metastases larger than two millimeters, so-called macrometastases, in one or two surgically removed sentinel nodes.
After gatekeeper surgery, patients were randomly assigned to axillary evacuation (which was previously the practice for everyone), or the rest of the armpit was left alone.

Most were treated with chemotherapy and/or anti-hormonal therapy plus radiation according to guidelines in each country.
More than one in three patients who underwent axillary dissection were found to have more metastases than the maximum of two in the sentinel nodes.
Post-processing seems to be enough.
It should have been the same for those who were allowed to keep the other lymph nodes.
However, relapses were equally common in both groups, suggesting that post-treatment is sufficient to remove any remaining tumor cells.
At the same time, a previous publication from the study showed that 13 percent of those who underwent axillary dissection reported serious or very serious problems with arm function, compared with 4 percent of those who had only the sentinel glands removed.


We assess that it is safe for patients to forgo axillary dissection if there are no more than two macrometastases in the sentinel nodes.
In these cases, axillary dissection is replaced with radiation therapy to the armpit, which causes less arm discomfort.
This has already been introduced into clinical practice in Sweden, says Jana de Boniface.
In these cases, axillary dissection is replaced with radiation therapy to the armpit, which causes less arm discomfort.
This has already been introduced into clinical practice in Sweden, says Jana de Boniface.
The study is called SENOMAC and is funded by the Swedish Research Council, the Swedish Cancer Society, the Nordic Cancer Union and the Swedish Breast Cancer Association.